Olecranon Fracture
Description/Cause
Prevalence/Risk Factors
Signs/Symptoms
Objective/Special Tests
Treatment/Interventions
References
1. Peach C, Ali A. Mini-symposium: the elbow: (iii) Proximal ulna fractures. Orthopaedics And Trauma [serial online]. October 1, 2012;26:310-315. Available from: ScienceDirect, Ipswich, MA. Accessed July 7, 2015.
2. Yi P, Weening A, Shin S, Hussein K, Tornetta P, Jawa A. Injury patterns and outcomes of open fractures of the proximal ulna do not differ from closed fractures. Clinical Orthopaedics And Related Research [serial online]. July 2014;472(7):2100-2104. Available from: MEDLINE Complete, Ipswich, MA. Accessed July 13, 2015.
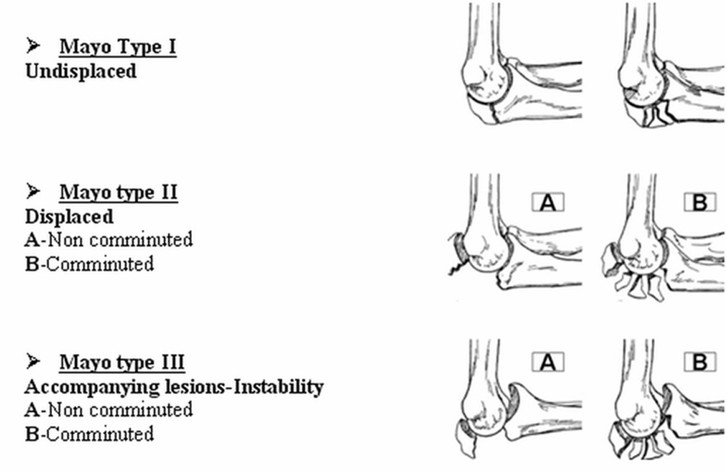
- Mayo Classification based on displacement, stability, and comminution:
- Mayo Type IA and IB: Undisplaced (<2 mm) fractures with no comminution (IA) or with comminution (IIB)
- Mayo type IIA: Stable fractures with O3 mm displacement, no comminution
- Mayo type IIB: Stable fractures with O3 mm displacement; comminution is present
- Mayo type IIIA: Unstable, displaced fracture–dislocations; no comminution is present
- Mayo type IIIB: Unstable, displaced fracture–dislocations; comminution is present
- Caused by direct or indirect trauma
- Direct: fall or blunt trauma on the posterior tip of the elbow
- Indirect: avulsion of the olecranon from eccentric triceps forces during a fall on a partially flexed elbow
Prevalence/Risk Factors
- Account for approximately 20% of fractures at the proximal forearm
- Most commonly seen with female adults
- Often seen in elderly: most often osteoporotic or osteopaenic
Signs/Symptoms
- Pain about the distal arm and elbow
- Swelling about the distal arm and elbow
- Displacement may have visible deformity
- Attempted motion may cause painful, bony crepitus
- Isolated olecranon fractures often lead to an inability to extend the elbow actively against gravity
Objective/Special Tests
- Radiographs
- Anteroposterior, true lateral, and oblique projections
- Palpation
- Assessment of soft tissue around the elbow
- ROM
- Should not be tested vigorously
- MMT
- Should not be tested vigorously
Treatment/Interventions
- Surgical treatments
- Techniques are chosen based on the fracture classification
- Non-Surgical
- Mayo Type I with intact extensor mechanism is treated with 2 weeks immobilization in midflexion and neutral forearm
- Rehabilitation
- Begin range of motion early
- Progressive rehabilitation of strengthening and range of motion
- Avoid flexion greater than 90 degrees, resisted elbow extension, or weight bearing until union is evident on radiograph
References
1. Peach C, Ali A. Mini-symposium: the elbow: (iii) Proximal ulna fractures. Orthopaedics And Trauma [serial online]. October 1, 2012;26:310-315. Available from: ScienceDirect, Ipswich, MA. Accessed July 7, 2015.
2. Yi P, Weening A, Shin S, Hussein K, Tornetta P, Jawa A. Injury patterns and outcomes of open fractures of the proximal ulna do not differ from closed fractures. Clinical Orthopaedics And Related Research [serial online]. July 2014;472(7):2100-2104. Available from: MEDLINE Complete, Ipswich, MA. Accessed July 13, 2015.
Acknowledgements:
David Funk, Student Physical Therapist at A.T. Still University
Ethan Hunke, Student Physical Therapist at A.T. Still University
Morgan Johnson, Student Physical Therapist at A.T. Still University
Ed Nheiu, Student Physical Therapist at A.T. Still University
Lindsay Walczak, Student Physical Therapist at A.T. Still University
Last edited: July 13, 2015
David Funk, Student Physical Therapist at A.T. Still University
Ethan Hunke, Student Physical Therapist at A.T. Still University
Morgan Johnson, Student Physical Therapist at A.T. Still University
Ed Nheiu, Student Physical Therapist at A.T. Still University
Lindsay Walczak, Student Physical Therapist at A.T. Still University
Last edited: July 13, 2015
