Distal Humerus Fracture
Description/Cause
Prevalence/Risk Factors
Signs/Symptoms
Objective/Special Tests
Treatment/Interventions
1. Wong A and Baratz M. Elbow Fractures: Distal Humerus. J Hand Surg. 2009; 34A:176–190.
- May be difficult to treat due to anatomic complexity, multi-fragmentary comminution/osteopenia, and a short distal segment
- Complex anatomy that articulates with both the radius and ulna, allowing for motion in multiple planes
- Comminution/osteopenia: may leave the metaphyseal-diaphyseal junction weak, making adequate stabilization weak
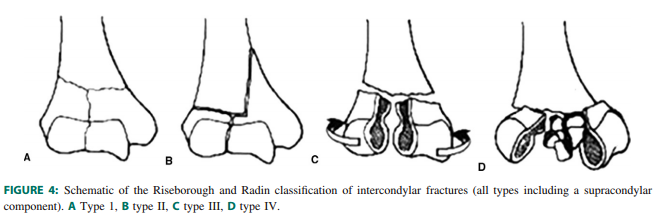
- Classification:
- Type I: extra-articular fracture
- Type II: fracture extends into the articular surface
- Type III: complete separation of the articular surface from the shaft
- Type IV: s severe comminution of the articular surface of one or both condyles
- A numerical 1-3 are given to types I-III to further classify the degree of comminution
- 1 is least comminuted
- 3 is most comminuted
- Caused by direct or indirect trauma
- Direct: the most common cause in older adults is falling
- Indirect: the most common cause in younger individuals is high energy trauma
Prevalence/Risk Factors
- Prevelance of 5.7/100,000
- Commonly seen in patients with osteoporosis
- Often seen in patients who participate in high impact activities
Signs/Symptoms
- Pain
- Swelling
- Difficult with movement at the elbow joint
- Visible deformity
Objective/Special Tests
- Radiographs
- Includes views of the wrist and shoulder to rule out other injuries
- CT (Computerized topography) scan
- 2-D CT allows for accurate assessment of the fracture in multiple planes and is often useful in surgical planning, but difficult when comminution or displacement are present
- 3-D provide a surface view of the anatomy and the ability to subtract the ulna and humerus from the image, allowing for more accurate characterization of the fracture
- Palpation
- MMT
- Range of motion
Treatment/Interventions
- Surgical:
- Considered the gold standard for displaced distal humerus fractures
- Regardless of approach, the ulnar nerve must be identified and protected
- Non-surgical:
- Used mainly for non-displaced fractures
- Immobilization for 2-3 weeks, followed by bracing
- Gentle motion should begin once the fracture is stabilized
- Rigid surgical fixation is preferred because range of motion can begin early and stiffness can be prevented
- Post-surgical rehabilitation
- Within 1-2 days active-assisted flexion and extension
- Within 6 weeks begin strengthening
- Daytime resting splint between therapy sessions to maintain forearm pronation and limit extension
1. Wong A and Baratz M. Elbow Fractures: Distal Humerus. J Hand Surg. 2009; 34A:176–190.
Acknowledgements:
David Funk, Student Physical Therapist at A.T. Still University
Ethan Hunke, Student Physical Therapist at A.T. Still University
Morgan Johnson, Student Physical Therapist at A.T. Still University
Ed Nheiu, Student Physical Therapist at A.T. Still University
Lindsay Walczak, Student Physical Therapist at A.T. Still University
Last edited: July 13, 2015
David Funk, Student Physical Therapist at A.T. Still University
Ethan Hunke, Student Physical Therapist at A.T. Still University
Morgan Johnson, Student Physical Therapist at A.T. Still University
Ed Nheiu, Student Physical Therapist at A.T. Still University
Lindsay Walczak, Student Physical Therapist at A.T. Still University
Last edited: July 13, 2015
